DSM5 ASD "Essentially Everyone Gets In"



http://www.psychiatry.org/practice/dsm
Many people have the idea that the "Diagnostic Criteria Sets" published, that can easily be found on the internet is all there is to the diagnostic text in the DSM, but there is much more that is copyrighted and not usually available to the general public in the "Descriptive Text" including: "Diagnostic Features"; "Subtypes and/or Specifiers"; "Recording Procedures"; "Associated Features and Disorders"; "Specific Culture, Age, and Gender Features"; "Prevalence"; "Course"; "Familial Pattern"; and "Differential Diagnosis."
The DSM is not designed as a cookbook to diagnose people; clinical experience is also required. However, there is no testing required to diagnose a person with an autism spectrum disorder in the US. Clinical experience, the DSM manual, and observation of the described behavioral impairments by a qualified professional with the credentials to diagnose, is all that is required for a diagnosis in the US.
Here is an example of the other information from the DSMIV-TR, not easily found with an internet search, linked below.
https://sites.google.com/site/gavinboll ... for-autism
https://sites.google.com/site/gavinboll ... -aspergers
I suppose the links are worth taking a look at....anyways that is what I was saying the DSM alone cannot be used to diagnose someone. Also, what testing would there be? There isen't an exact obvious simple difference between neurotypical and autistic brains so even if there was some sort of brain scan added as a required test for diagnoses it wouldn't work to well I don't think.
Some professionals, more commonly neuro-psychiatrists, use a number of related "paper" tests that provide additional measures of the diagnostic features.

Is there anything that can be done to stop this change? It was put forward as a proposal and roundly rejected by most (as far as I have seen), yet it goes ahead. What strikes me most is that the panel is not listening to the very informed views of people with Aspergers.
The whole subject is misunderstood for as long as we remain largely clueless as to the brain. It rather annoys me that so many people have career interests in basically screwing around with peoples lives. My own included.
My genetic relatives are Aspies that are clearly not out and out Autistic and lumping them together is just lazy ignorance by people who have no idea how ignorant they actually are.
My belief is that they relate but Autism proper is far more genetic and less environmental. They manifest as a spectrum but ultimately are to be treated differently.
The whole subject is misunderstood for as long as we remain largely clueless as to the brain. It rather annoys me that so many people have career interests in basically screwing around with peoples lives. My own included.
My genetic relatives are Aspies that are clearly not out and out Autistic and lumping them together is just lazy ignorance by people who have no idea how ignorant they actually are.
My belief is that they relate but Autism proper is far more genetic and less environmental. They manifest as a spectrum but ultimately are to be treated differently.
There were three public commenting periods, where some adjustments were made in revisions of the one consolidated autism spectrum disorder.
The final revision of the DSM5 has been approved by the APA board of trustees and there is no turning back from that final revision at this point, but always the potential for new revisions in the future after the current final revision is published in 2013. Part of the reason a change was made from using Roman numerals in this revision is so more frequent future minor revisions could be made like DSM-5.1,5.2, etc.
I think it is highly unlikely that we will ever see the term Asperger's again, used as a diagnostic label in a DSM5 future revision, but I don't expect the same for all of the other diagnostic manuals more commonly used in other countries, that do still continue to include Asperger's as a diagnosis.
Verdandi
Veteran
![]()

Joined: 7 Dec 2010
Age: 54
Gender: Female
Posts: 12,275
Location: University of California Sunnydale (fictional location - Real location Olympia, WA)
ICD-11 calls Asperger's Syndrome Social Reciprocity Disorder. It lists Asperger's as a synonym.
I recall someone involved with the change to ASD saying that the term "Asperger's" would appear as a description of a particular presentation of autism.
So, it looks like "Asperger's Syndrome" as the name for a diagnostic label is going away, but the use of it to describe some people under those labels may remain.
Verdandi
Veteran
![]()
Joined: 7 Dec 2010
Age: 54
Gender: Female
Posts: 12,275
Location: University of California Sunnydale (fictional location - Real location Olympia, WA)
You are addressing the issue, but I would argue that you're not being objective.
So, you're already applying a bias here, as you have not stopped to determine whether the usage of "neurotypical" fit the original intent, or if it's used with this more recent concern. I do not recall that neurotypical was ever presented with a "scientific basis" as opposed to labeling the fact that being autistic tends to put one at a disadvantage for a variety of reasons, not all of them directly derived from being autistic. It's more appropriate to describe it as a sociological term.
My point about "typical" referring to a range of presentations was not to say that neurotypical has a scientific basis, but to say that it does not refer to exactly one kind of brain.
Yes, she stated that more than half the people would not meet the DSM-IV criteria for Asperger's. There's a study that was linked on the rationale page for the ASD DSM-V entry that explained that most people diagnosed with AS would not meet the criteria for AS because they meet the criteria for autism. I am still not convinced by your interpretation that she was being negative or dismissing people as not really being autistic. I am not defending her because I care about her reputation, I am simply explaining my interpretation of what I read.
Neurotypical isn't a diagnosis. It's a social category. Sometimes applying it will turn out to be wrong. That is a risk one takes when trying to find ways to talk about how people fit into different categories.
Ne'eman and the GRASP director may not communicate that smoothly in all situations and all contexts. I was very "articulate" in explaining myself when I was diagnosed with AS, but the night before I had written notes and essentially recited those notes at the appointment. At other times, I have been unable to string two coherent sentences together because I was unprepared and could not assemble what I determined to be something appropriate to say. My ability to communicate verbally ranges between "articulate" and "mute."
Neither do I, if that is what she is saying. However, the statistics say that referring to her as "neurotypical" is a safe bet.

Aspergers should stay right where it is IN THE DSM
until they study it more. Why? Two names.
Adam Lanza and Nancy Lanza
I think there was a catalyst for this act horrifying violence.
We as a society need to research, learn and help more, more, more.
removing diagnostic criteria is no way to help!
Verdandi
Veteran
![]()
Joined: 7 Dec 2010
Age: 54
Gender: Female
Posts: 12,275
Location: University of California Sunnydale (fictional location - Real location Olympia, WA)
Lacking an actual plague of autistic spree killers, that strikes me as a bit melodramatic.
Anyway, Adam's brother said he was diagnosed with a form of autism or a personality disorder.
Also, the assumption that research will stop because the diagnosis changed is unfounded. There are few things autism specialists seem to love more than endlessly researching autism, even to the exclusion of providing concrete services for autistic people.
I recall someone involved with the change to ASD saying that the term "Asperger's" would appear as a description of a particular presentation of autism.
So, it looks like "Asperger's Syndrome" as the name for a diagnostic label is going away, but the use of it to describe some people under those labels may remain.
That's interesting, thanks for that information; are you aware of any changes in the Gillberg Criteria? As far as I know there has been no suggestion that criteria is changing.
You are addressing the issue, but I would argue that you're not being objective.
So, you're already applying a bias here, as you have not stopped to determine whether the usage of "neurotypical" fit the original intent, or if it's used with this more recent concern. I do not recall that neurotypical was ever presented with a "scientific basis" as opposed to labeling the fact that being autistic tends to put one at a disadvantage for a variety of reasons, not all of them directly derived from being autistic. It's more appropriate to describe it as a sociological term.
My point about "typical" referring to a range of presentations was not to say that neurotypical has a scientific basis, but to say that it does not refer to exactly one kind of brain.
Yes, she stated that more than half the people would not meet the DSM-IV criteria for Asperger's. There's a study that was linked on the rationale page for the ASD DSM-V entry that explained that most people diagnosed with AS would not meet the criteria for AS because they meet the criteria for autism. I am still not convinced by your interpretation that she was being negative or dismissing people as not really being autistic. I am not defending her because I care about her reputation, I am simply explaining my interpretation of what I read.
Neurotypical isn't a diagnosis. It's a social category. Sometimes applying it will turn out to be wrong. That is a risk one takes when trying to find ways to talk about how people fit into different categories.
Ne'eman and the GRASP director may not communicate that smoothly in all situations and all contexts. I was very "articulate" in explaining myself when I was diagnosed with AS, but the night before I had written notes and essentially recited those notes at the appointment. At other times, I have been unable to string two coherent sentences together because I was unprepared and could not assemble what I determined to be something appropriate to say. My ability to communicate verbally ranges between "articulate" and "mute."
Neither do I, if that is what she is saying. However, the statistics say that referring to her as "neurotypical" is a safe bet.
http://www.ncbi.nlm.nih.gov/pubmed/17927727
This is the study that was referenced in the rationale, but it studys children not adults. If Lord was referring to this in context with the adults that use Aspergers and want to keep the label for a sense of community that would not work in the real world because Autistic Disorder currently requires one of three developmental delays or abnormal functioning before age 3, and many of these adults self diagnosed or diagnosed with Asperger's have no record of developmental delays or abnormal function before age 3. Many were not diagnosed until early adulthood or later.
The DSM5 definition of Autism Spectrum Disorder accommodates that requirement and concern that was voiced by individuals diagnosed later in life, by describing symptoms in early childhood that don't present fully until social demands exceed the capacity to meet them.
Lord has no idea how many adults identifying with the label as a source of community were diagnosed with this kind of developmental history as adults. And I'm sure she is clearly aware of the lack of research among adults with all forms of autism in the US. You could be correct that she was using that rationale, but if so it is still not a "rational" one.
I identified in my post that my discussion was not based on what the intent of the specific person that used the term NT was per earlier or later versions of the definition. You didn't quote that part of my post.
As I stated several times I was only referring to the more recent usage of Neurotypical that some individuals use to to describe people with "fully normal neurology" as referenced in Wiki. You have yet to use it in that manner, so I am not suggesting it has anything to do with your personal definition of it.
There are no statistics on this description of fully normal neurology because it has not been defined or studied in the general population.
Obviously when people attempt to assess people with this imaginary status of neurology with an armchair analysis in an individual they are not diagnosing a real diagnosis they are diagnosing or assessing an imaginary status of fully normal neurology that does not exist in the real world.
It's okay to imagine a lot of people out their with this imaginary quality of having "fully normal neurology", but it is impossible to accurately assess or diagnose that imaginary status of neurology in an individual from a casual armchair analysis. Particularly when one considers that there is no way to determine an imaginary status objectively.
Some professionals with extensive clinical experience with Asperger's will not assess a diagnosis of Asperger's syndrome in an adult until they have observed the patients over the course of many appointments, because of the difficulty that people like the director of grasp present in how seamlessly they interact with others in what most would consider stressful social situations.
That's going to be that much more difficult for the patient in the future when one doesn't have the opportunity for their diagnosing professional to bypass the optional criterion for social-emotional reciprocity, non-verbal communication impairments, or developing and maintaining friendships, none of which were mandatory requirements by themselves in the DSMIV-TR. The director of grasp was an international diplomat; it doesn't get much more adaptive than that, at least in the arena of social communication with others. The same applies to Ne'eman, however neither of them faced the mandatory criterion of the DSM5.
Eventually ASD may not be a diagnosable invisible disability for some, because some may be "diagnosed" by professionals with the definition of neurotypical that you provided earlier because they do not present significant observable impairments in either social-emotional reciprocity or non-verbal impairments or other previously optional criterion per what you described as characteristics of "neurotypicals" who also do not present these criterion symptoms.
That's part of the issue, much of what you described as the observable impairments of a person on the spectrum are symptoms but they are not currently mandatory symptoms for a diagnosis. The definition you provided of neurotypical might eventually work much better for those diagnosed as adults when the DSM5 is in effect for a decade or so.
However, that's not going to help the adults that didn't get diagnosed with the invisible disability and are "assessed" as "neurotypical" per the definition you provided. The "neurotypical" vs. Autistic observations in the research linked above for children would probably work just fine per the definition you provided of neurotypical vs. these children that haven't had an opportunity to socially adapt over the course of decades.
Hopefully the quotation marks clarified it, but in case they didn't to clarify I'm not suggesting that any professionals are literally diagnosing anyone with an imaginary condition.
This is the part of it that Lord does not appear to be acknowledging and cannot reasonably acknowledge because there is no significant research in this adult area. She is still looking at these adults as children, if she used the link above to justify her comment.
Verdandi
Veteran
![]()
Joined: 7 Dec 2010
Age: 54
Gender: Female
Posts: 12,275
Location: University of California Sunnydale (fictional location - Real location Olympia, WA)
I recall someone involved with the change to ASD saying that the term "Asperger's" would appear as a description of a particular presentation of autism.
So, it looks like "Asperger's Syndrome" as the name for a diagnostic label is going away, but the use of it to describe some people under those labels may remain.
That's interesting, thanks for that information; are you aware of any changes in the Gillberg Criteria? As far as I know there has been no suggestion that criteria is changing.
I am unaware of any changes to it. I wouldn't be surprised if some diagnosticians continued to use it and gave SRD or ASD diagnoses with the note that it is "Asperger's."
HDLMatchette
Deinonychus
![]()
Joined: 15 Dec 2012
Age: 29
Gender: Male
Posts: 338
Location: Fuquay-Varina, North Carolina

I really wish people who claim the existence of such a 'crowd' would either give me evidence that they exist, or stop perpetuating this myth.
There are a number of self-diagnosed aspies. As far as I've seen, their behavior online does not appear to be particularly different from officially diagnosed aspies. In fact, the most 'vocal' aspies I've seen all have official diagnoses.
Also, I don't get what is supposed to be wrong with making an identity out of the label. It's just recognizing the reality that AS impacts on a number of areas central to an individual's personality. If NTs get to make an identity out of being a 'people person' or 'party animal', what reason is there to deny that AS can be an identity as well?
What real and obvious distinction? Ask 15 people what the difference between HFA and AS is, and you'll get fifteen different answers.
And DSM-IV AS doesn't exist - everyone who meets the social criteria (shared between autism and AS) also meets the communication criteria (autism only) and therefore technically is autistic rather than AS according to the DSM. (You don't need a language delay for autism, you can meet communication criteria by having pragmatic language issues or echolalia even if your speech milestones were normal.)
I really wish people who claim the existence of such a 'crowd' would either give me evidence that they exist, or stop perpetuating this myth.
There are a number of self-diagnosed aspies. As far as I've seen, their behavior online does not appear to be particularly different from officially diagnosed aspies. In fact, the most 'vocal' aspies I've seen all have official diagnoses.
Also, I don't get what is supposed to be wrong with making an identity out of the label. It's just recognizing the reality that AS impacts on a number of areas central to an individual's personality. If NTs get to make an identity out of being a 'people person' or 'party animal', what reason is there to deny that AS can be an identity as well?
What real and obvious distinction? Ask 15 people what the difference between HFA and AS is, and you'll get fifteen different answers.
And DSM-IV AS doesn't exist - everyone who meets the social criteria (shared between autism and AS) also meets the communication criteria (autism only) and therefore technically is autistic rather than AS according to the DSM. (You don't need a language delay for autism, you can meet communication criteria by having pragmatic language issues or echolalia even if your speech milestones were normal.)
Swedo in her comment was talking about a relatively few number of vocal individuals that were self-diagnosed. Lord in her comment was referring to over half of those that use Aspergers, but as Verdandi pointed out she could have been referring to the study I linked that suggested over half of a sample group of children who met the requirements for Asperger's disorder would have met the requirements for Autistic Disorder, however that is based on children not the adult demographic that is the population in question in both of the statements from the working group committee. Many of those children in the linked study were inappropriately diagnosed with Aspergers syndrome with intellectual development delays, and language delays. The full study is linked below:
http://onlinelibrary.wiley.com/doi/10.1 ... 1232.x/pdf
The GRASP organization if that was the organization that Swedo referred to, supports individuals that self diagnose. The same is true for other vocal self-advocates and other small vocal self-advocacy organizations spread out across the US.
There are thousands of individuals on this site registered as self-diagnosed and at least some have gone on to start very popular facebook autism online communities, one of which has over 20,000 likes. Several that report they don't have official documentation for a diagnosis are authors of books. Swedo referenced one of these self-diagnosed authors with her mention of the Aspie.com site.
Most of these individuals if not members of Grasp are highly supportive of that organization. If one doesn't visit facebook much they are missing some extremely vocal self-advocates that are either self diagnosed, or admit they have no official documentation for a diagnosis. I don't know specifically which individuals Swedo was referring to, but I certainly could name a relatively small group of highly vocal self-advocates reporting themselves as self-diagnosed, meeting the description Swedo provided.
I'm not sure if you have seen the diagnostic features from the DSMIV-TR linked below, but the two examples below of just one criterion describes the severity levels differentiated between the two disorders. Technically if one uses the criteria with the more severe examples of diagnostic features for Autistic Disorder to diagnosis someone with Asperger's syndrome, that also have an assessed delay or abnormal functioning in social interaction, abnormal functioning in language or imaginative play before the age of three and at least one of the communication impairments described in autistic disorder they can be diagnosed technically correct with a condition that overall is not described as Aspergers syndrome in the diagnostic features text in the DSMIV-TR.
However, that is an issue of the overlap described in the two disorders in the criterion without strict severity guidelines; that is the responsibility of the individuals that designed the DSMIV and at least some professionals that may not be paying close attention to the differences in the diagnostic features described in the DSMIV-TR when they diagnose individuals.
There are these potentials of misdiagnosis, the overlap of the severity of elements in the criterion in both disorders, including some of the elements in the communication criteria for Autistic Disorder that may also be met with no requirement among those diagnosed with Asperger's syndrome.
But, the potential for developmental delays or abnormal function in social interaction, abnormal function of language, and abnormal function of imaginative play before age three; all technically allowed in a diagnosis of Asperger's syndrome are elements, including clinically significant delays in language not acceptable in a diagnosis of Asperger's syndrome, of which one is a mandatory requirement to meet the current diagnostic requirements for autistic disorder. The potential that an adult going in for a diagnosis would have a medical record of one of these specific required impairments before age 3 is not likely.
More concisely put, currently Autistic Disorder has a mandatory requirement for one of these criterion elements of abnormal functioning or developmental delays before the age of three, and Asperger's does not.
So, there is no way one can suggest with certainty and no research to back up a suggestion that the majority of individuals diagnosed in adulthood with Asperger's or PDDNOS would meet the current diagnostic requirements in the DSM-IV-TR for Autistic Disorder.
Whether or not a diagnosing professional accepts the word of an adult seeking a diagnosis without a history from a caretaker, family member instead of medical records in the new diagnostic mandatory criterion for DSM5 autistic spectrum disorder that more loosely describes "symptoms" that must occur in early childhood and fully present themselves when social demands exceed individual capacity for adaptation is speculative at best at this point, with no real life studies in the clinical diagnostic environment for adults and none planned at this point. There is potential that the DSM5 diagnostic features, when published for those that can gain access to them, might provide more details of guidance for professionals on this specific early childhood criterion requirement.
Delays and abnormal functioning criterion from the DSM-IV-TR Autistic Disorder Criteria set, quoted below. The link also provides the DSM-IV-TR text of the criteria sets for Autistic Disorder, Asperger's Disorder, and Pervasive Development Disorder Not otherwise specificed (PDDNOS)
http://www.tidelandscounseling.com/dsm- ... -disorders
(A) social interaction
(B) language as used in social communication
(C) symbolic or imaginative play
https://sites.google.com/site/gavinboll ... for-autism
https://sites.google.com/site/gavinboll ... -aspergers
From the Asperger's Disorder DSM-IV-TR Diagnostic Features text:
From the Autistic Disorder DSM-IV-TR Diagnostic Features text:
The potential of actual diagnostic differences even in one diagnosis, autistic disorder, not even taking into account different examples of severity of symptoms listed in the diagnostic features section is 2027 diagnostic combinations based on the 6 of 12 current DSMIV-TR criterion requirements of autistic disorder linked and illustrated below.
There is the actual potential that two people currently diagnosed with Autistic Disorder can be diagnosed with six completely different criterion, as illustrated below. That number of criteria referenced is reduced, consolidated, and more broadly described in the DSM5. The difference in diagnostic criterion combinations is huge though, with 11 in the new criteria as opposed to 2027 in the existing diagnostic criteria.
While that is an overstatement from raw numbers, not taking into account the consolidation of or broadening of criterion descriptions for range of severity of examples provided in the last public revision of the DSM5, the impact on diagnosis in the real world, in the future, with this new criteria, particularly among those diagnosed later in life, shouldn't be minimized by Lord and associates, because of the lack of research in this area, and these factors that the DSM5 committee did not openly address with the public.
http://crackingtheenigma.blogspot.com/2 ... o-get.html
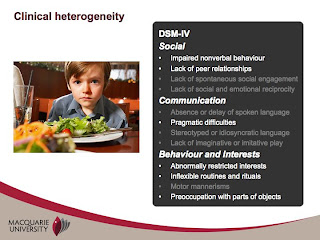
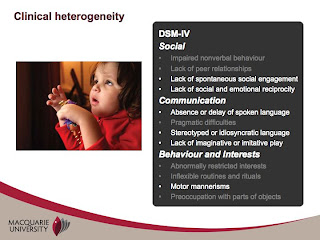
The latest publicly published Revision of the DSM5, criteria set for Autism Spectrum Disorder is linked and quoted below for the individual that was wondering what the DSM5 was. The acronym stands for Diagnostic and Statistical Manual of Mental Disorders. It is the Diagnostic Manual supported by the American Psychiatric Association APA, used by most diagnosing professionals in the US, and required for classification/coding purposes for hospitals, clinics, and insurance companies.
http://en.wikipedia.org/wiki/Diagnostic ... _Disorders
An individual must meet criteria A, B, C and D:
A. Persistent deficits in social communication and social interaction across contexts, not accounted for by general developmental delays, and manifest by all 3 of the following:
Deficits in social-emotional reciprocity; ranging from abnormal social approach and failure of normal back and forth conversation through reduced sharing of interests, emotions, and affect and response to total lack of initiation of social interaction.
Deficits in nonverbal communicative behaviors used for social interaction; ranging from poorly integrated- verbal and nonverbal communication, through abnormalities in eye contact and body-language, or deficits in understanding and use of nonverbal communication, to total lack of facial expression or gestures.
Deficits in developing and maintaining relationships, appropriate to developmental level (beyond those with caregivers); ranging from difficulties adjusting behavior to suit different social contexts through difficulties in sharing imaginative play and in making friends to an apparent absence of interest in people
B. Restricted, repetitive patterns of behavior, interests, or activities as manifested by at least two of the following:
Stereotyped or repetitive speech, motor movements, or use of objects; (such as simple motor stereotypies, echolalia, repetitive use of objects, or idiosyncratic phrases).
Excessive adherence to routines, ritualized patterns of verbal or nonverbal behavior, or excessive resistance to change; (such as motoric rituals, insistence on same route or food, repetitive questioning or extreme distress at small changes).
Highly restricted, fixated interests that are abnormal in intensity or focus; (such as strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
Hyper-or hypo-reactivity to sensory input or unusual interest in sensory aspects of environment; (such as apparent indifference to pain/heat/cold, adverse response to specific sounds or textures, excessive smelling or touching of objects, fascination with lights or spinning objects).
C. Symptoms must be present in early childhood (but may not become fully manifest until social demands exceed limited capacities)
D. Symptoms together limit and impair everyday functioning
Last edited by aghogday on 16 Dec 2012, 9:46 pm, edited 1 time in total.

But even with those potentials of misdiagnosis and the overlap of the criterion, those developmental delays in social interaction or abnormal functioning in social interaction, language development and imaginative allowed before the age of 3 for a diagnosis of Asperger's syndrome and autistic disorder, are not issues that adults going in for a diagnosis have any record of.
(A) social interaction
(B) language as used in social communication
(C) symbolic or imaginative play
https://sites.google.com/site/gavinboll ... for-autism
https://sites.google.com/site/gavinboll ... -aspergers
From the Asperger's Disorder DSM-IV-TR Diagnostic Features text:
Quote:
"Lack of social or emotional reciprocity may be present (e.g.,not actively participating in simple social play or games, preferring solitary activities, or involving others in activities only as tools or "mechanical" aids)(Criterion A4). Although the social deficit in Asperger's Disorder is severe and is defined in the same way as in Autistic Disorder, the lack of social reciprocity is more typically manifest by an eccentric and one-sided social approach to others (e.g.,pursuing a conversational topic regardless of other' reactions) rather than social and emotional indifference."
From the Autistic Disorder DSM-IV-TR Diagnostic Features text:
Quote:
"Lack of social or emotional reciprocity may be present (e.g.,not actively participating in simple social play or games, preferring solitary activities, or involving others in activities only as tools or "mechanical" aids)(Criterion A1d) Often an individual's awareness of others is markedly impaired. Individuals with this disorder may be oblivious to other children (including siblings), may have no concept of the needs of others, or may not notice another person's distress."
This is where I get confused.
My social problems sound more like what is described for "autism," and yet I'm DXed with Aspergers.
Do the sub-types of Aspergers described by Lorna Wing factor into this?
_________________
"If we fail to anticipate the unforeseen or expect the unexpected in a universe of infinite possibilities, we may find ourselves at the mercy of anyone or anything that cannot be programmed, categorized or easily referenced."
-XFG (no longer a moderator)


